


A patient presented with a rapidly deteriorating pain in his right hip which he had had for the past 6 months.
The patient presented with a rapidly deteriorating pain in his right hip which he had had for the past 6 months. Ten year ago, he underwent a left hybrid total hip replacement. It was noticed at the time of surgery that the cartilage had an abnormal blue tinge, and this raised the possibility of the patient having metabolic bone disease. The patient had an older brother with a confirmed diagnosis of alkaptonuria with a typical radiographic finding of the spine and other large joints. As an infant, it was noted that the nappies had an abnormal colouration. However, a diagnosis of alkaptonuria had not been made. There was no other relevant medical history. The diagnosis was later confirmed by doing an urine analysis for homogentisic acid. Plain radiographs of the hips taken with a 6 month gap showed a rapidly progressive destructive arthropathy affecting both the acetabular and femoral components of the right hip. MRI investigation showed extensive destruction of the right femoral head with a thickened synovium. Heterogenous areas within the right hip were consistent with fragmentation and destruction of the cartilage with extensive interarticular debris.
Alkaptonuria is a rare, inherited enzyme deficiency of homogentisic acid oxidase causing the accumulation of homogentisic acid when tyrosine and phenylalanine are metabolized. This is excreted in the urine and is oxidized on standing to form a black pigment. Homogentisic acid has a predilection for connective tissue and cartilage. Abnormal pigmentation of the sclera, ears and skin is usually evident by the time a person reaches his twenties. Clothes may be stained due to excessive pigment being excreted in the sweat. Alkaptonuria is a multisystem disorder affecting the cardiovascular system with aortic valve disease (mean age:54), coronary artery calcification (mean age:59), renal stones (mean age:64) and arthropathy leading to joint replacements (mean age:55) . The first manifestations of musculoskeletal symptoms are in the 30s with pain and stiffness of the back . The hips, knees and shoulders are usually involved some years later. The radiographic changes are similar to that of premature osteoarthritis (OA). Loss of articular cartilage and bony sclerosis are prominent. Features that favour alkaptonuria over OA are small or absent osteophytes, collapse and fragmentation with loose intra-articular loose bodies and tendon calcification and ossification.
Alkaptonuria of the right hip.





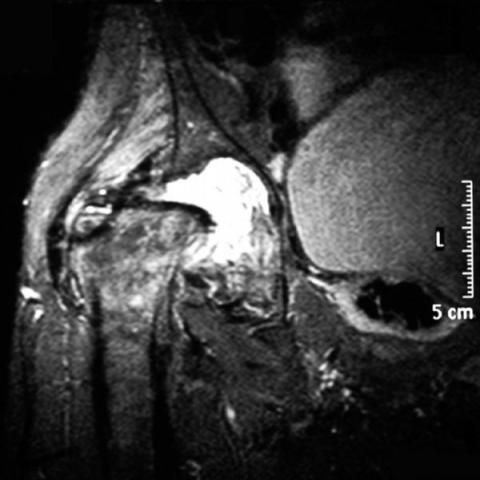
According to the provided X-ray and MRI images, the right hip joint has already undergone artificial joint replacement. The surrounding bone shows significant sclerosis, with some cartilage surfaces and bone structures exhibiting collapse and fragmentation, and the joint space is severely narrowed. Compared to conventional degenerative osteoarthritis, there appear to be relatively fewer or smaller osteophytes (bone spurs), more pronounced trabecular sclerosis, and focal or patchy density abnormalities in certain areas. MRI images indicate complex signals in the soft tissue around the hip joint; calcification or small patchy low-signal areas can be seen around certain soft tissues or tendons, and there are also small patchy shadows around the joint that resemble loose bodies. Overall, these findings are consistent with severe joint degeneration and abnormal calcification/ossification in the surrounding soft tissue.
Considering the patient’s long-term (>6 months) worsening hip pain, clinical indication of a hereditary metabolic disorder (Alkaptonuria), and radiological signs of significant cartilage destruction and collapse with fewer osteophytes, combined with soft tissue calcification, the most likely diagnosis is:
Severe hip arthropathy caused by Alkaptonuria (Black Urine Disease).
The patient has already undergone hip joint replacement, consistent with the clinical feature that degenerative changes associated with Alkaptonuria often necessitate relatively early joint replacement.
Given that the patient has undergone hip replacement and has cartilage and connective tissue damage caused by Alkaptonuria, a gradual, individualized rehabilitation plan following the FITT-VP principle (Frequency, Intensity, Time, Type, Progression, and Volume) is recommended.
If there is any concern about bone fragility or cardiopulmonary function, training intensity and frequency should be carefully adjusted under medical or therapeutic supervision to avoid falls or cardiovascular complications.
This report is a reference analysis based on currently available imaging data and medical history. It does not replace an in-person consultation or professional medical diagnosis and treatment advice. If further evaluation is needed, please consult a specialist for appropriate examinations and follow-up.
Alkaptonuria of the right hip.